





How to prevent the nerve impinge during dental implantation?
 @Download from the Doe report
@Download from the Doe report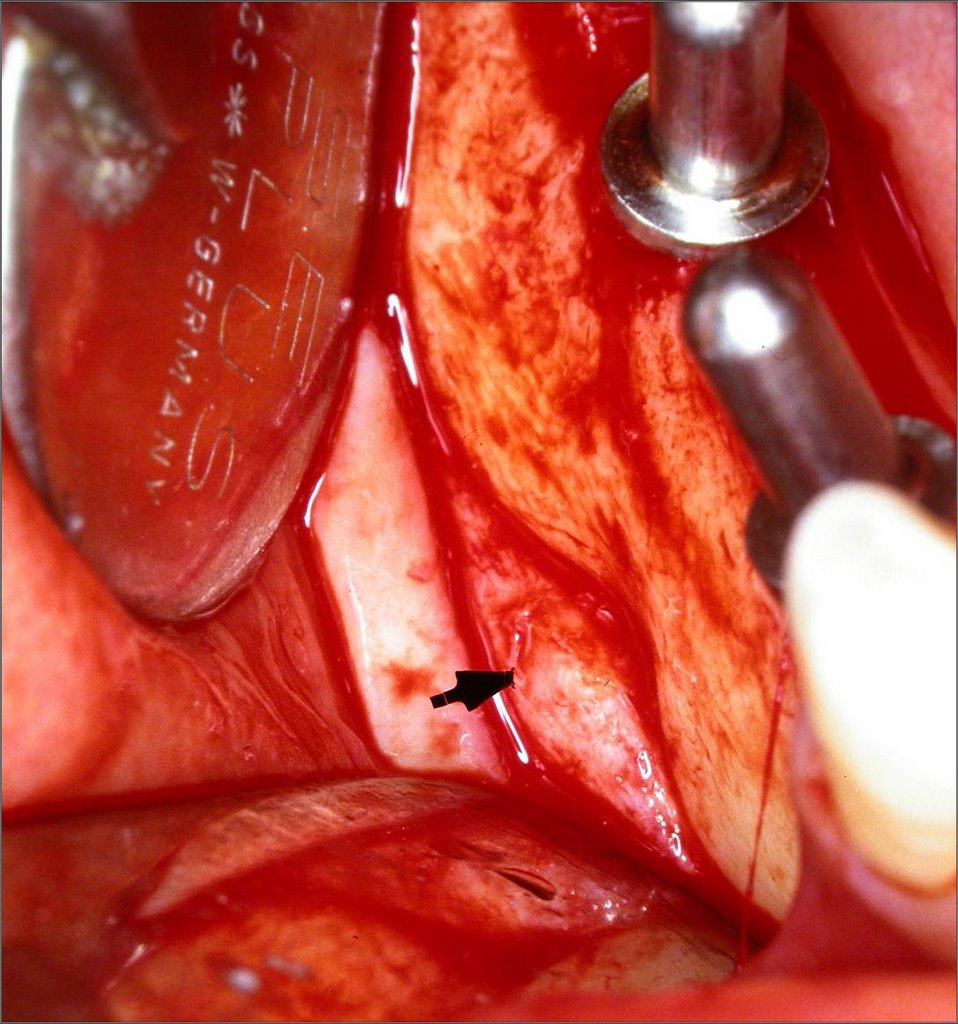 The inferior dental nerve is at risk of damage during removal of lower third molars, during apicectomy of lower premolar and molar teeth, the placement of intraoral implants and soft tissue surgery around the mental foramen, especially in the elderly where the mental nerve may lie at or close to the alveolar crest.
The inferior dental nerve is at risk of damage during removal of lower third molars, during apicectomy of lower premolar and molar teeth, the placement of intraoral implants and soft tissue surgery around the mental foramen, especially in the elderly where the mental nerve may lie at or close to the alveolar crest.Intraoral implants, particularly mandibular endosseous implants are emerging as yet another cause of litigation resulting from iatrogenic nerve damage. Preoperative planning and imaging together with the careless siting of endosseous implants may damage the inferior alveolar nerve either within the mandibular canal or after its exit from the mental foramen. The prevalence of altered inferior alveolar nerve sensation following the placement of mandibular endosseous implants has been reported to be as high as 36% of which 23% of cases were transient and 13% of cases were persistent at 6 months or more post implant placement. Although uncommon, transient lingual nerve paraesthesia has also been reported where mandibular endosseous implants have perforated the lingual cortical plate. Inferior alveolar nerve repositioning to facilitate the placement of endosseous implants posterior to the mental foramen is associated with a very high incidence of temporary inferior alveolar nerve damage. In one series inferior alveolar neurosensory dysfunction was present in 70% of patients at 1 week before falling to 20% at 6months and 0% at 1 year postoperatively. However, the technique enables the placement of more and longer implants resulting in increased prosthesis strength and stability and has a lower permanent dysaesthesia rate than when a non-transposed nerve has been accidentally damaged by drilling or implant placement. If such a technique is to be used it is vital that the patient is fully informed about the possibilityof temporary and permanent inferior alveolar nerve paraesthesia.
#1. The surgeon should always be cognizant of the location of the mental foramen. The mental foramen lies on the same vertical line defined by the pupil, infraorbital foramen and the second bicuspid tooth.
@Morphometric Analysis of Implant-Related Anatomy in Caucasian Skulls
Journal of Periodontology
2004, Vol. 75, No. 8, Pages 1061-1067
Rodrigo F. Neiva et al.
The most common location of the MF (mental foramen) in relation to teeth was found to be below the apices of mandibular premolars. The mean MF-H was 3.47 ± 0.71 mm and the mean MF-W was 3.59 ± 0.8 mm. The mean distance from the MF to other anatomical landmarks were: MF-CEJ = 15.52 ± 2.37 mm, MF to the most apical portion of the lower cortex of the mandible = 12.0 ± 1.67 mm, MF to the midline = 27.61 ± 2.29 mm, and MF-MF = 55.23 ± 5.34 mm.
 ^^^88% cases .. anterior loop of mental bundle >4.13mm
^^^88% cases .. anterior loop of mental bundle >4.13mm#2. @Evaluation of the tracings for implants in panoramic radiographs before dental implaantation

***A Website special for Oral Nerve Injury
http://www.sciential.net/cgi-bin/dcforum/dcboard.cgi?az=post&forum=DCForumID9&om=113&omm=0
Listen!!! @A completely terrified statement of inferior alveolar nerve injury following a dental implant from a patient
@Commends from OsseoNews for a case about special pain after dental implant impinged the nerve
posted by Ajou Huang @ 6:00 pm
1 comments
![]()
![]()
1 Comments:
It is very important to note the mental nerve bundle, especially anterior loop.
Anterior loop varities are many.
Bewell dont'touch any more.
Post a Comment
<< Home