





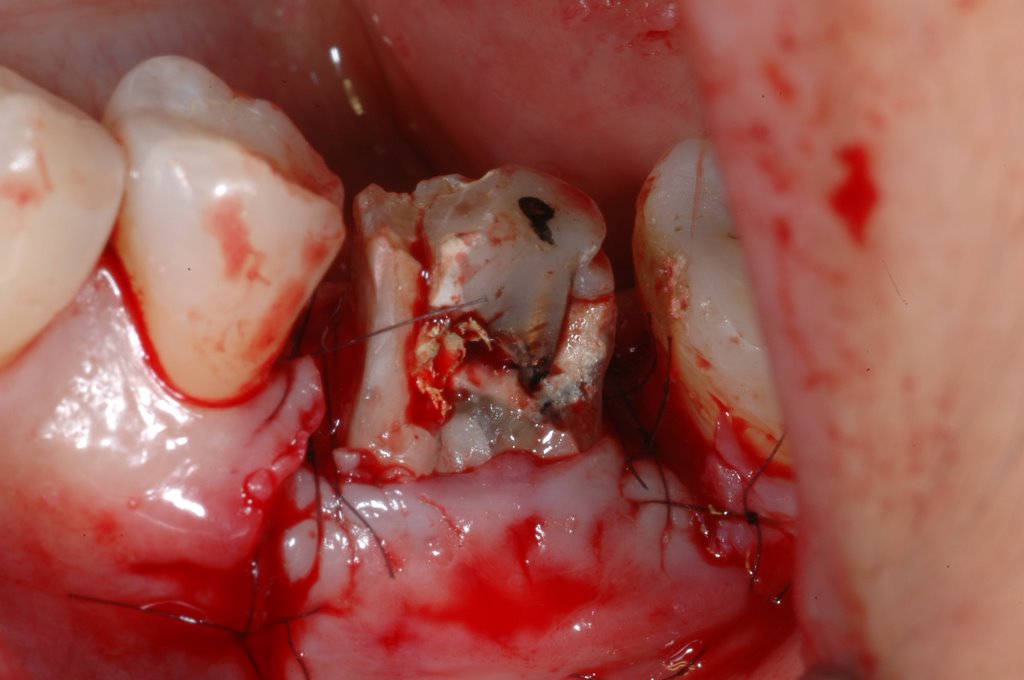
Glass Ionomer filling into severe furcation invlovement of Molar tooth
 Treatment of Class III furcation has historically been less than predictable. Long-term studies have demonstrated poor survival rates of teeth with advanced furcation involvement. Although multiple treatment modalities have been attempted to retain teeth with severe furcation invasion, clinical success has not been predictable. Treatment attempts range from non-surgical therapy, furcation obliteration,surgery to increase access to the furcation, root resections, tunnel procedure, guided tissue regeneration, and a combination of graft materials, membranes, and coronally positioned flaps. Regenerative techniques that have been successful in the treatment of Class II mandibular furcation involvements have been less predictable when performed in Class III situations. In the past restorative materials have been used to obliterate furcation; the goal was to improve plaque control by eliminating the anatomic niches within the furcation where bacteriacan accumulate. Also, in the past polymericreinforced zinc oxide-eugenol (IRM), amalgam,glass ionomer, and resin ionomer restorative materials were utilized to fill Class III furcation invasions.
Treatment of Class III furcation has historically been less than predictable. Long-term studies have demonstrated poor survival rates of teeth with advanced furcation involvement. Although multiple treatment modalities have been attempted to retain teeth with severe furcation invasion, clinical success has not been predictable. Treatment attempts range from non-surgical therapy, furcation obliteration,surgery to increase access to the furcation, root resections, tunnel procedure, guided tissue regeneration, and a combination of graft materials, membranes, and coronally positioned flaps. Regenerative techniques that have been successful in the treatment of Class II mandibular furcation involvements have been less predictable when performed in Class III situations. In the past restorative materials have been used to obliterate furcation; the goal was to improve plaque control by eliminating the anatomic niches within the furcation where bacteriacan accumulate. Also, in the past polymericreinforced zinc oxide-eugenol (IRM), amalgam,glass ionomer, and resin ionomer restorative materials were utilized to fill Class III furcation invasions.@Potential advantages of an occlusive barrier such as glass ionomer include:
• Ease of placement
• Does not require a suture for stability
• Elimination of a second stage procedure for retrieval of the membrane since it is permanently bonded
• Long junctional epithelial attachment to the glass ionomer
• Does not require complete coverage by the gingival flap
• Bacteriostatic due to fluoride release
• Lower cost
The use of a glass ionomer to regenerate the attachment apparatus in the treatment of advanced furcation involvement was not the goal of the treatment. There was no intention to regenerate any tissue, hard or soft. The goal of selecting this mode of therapy was simply to retain hopeless molars with advanced furcation defects.
A case report for filling Fuji II LC into Mandibular Cl III molar FI and final procelain to metal crown restoration: Surgery by Dr. Perio




 @PostSx 4 months....
@PostSx 4 months....
.12.jpg)
posted by Ajou Huang @ 10:42 pm
0 comments
![]()
![]()
0 Comments:
Post a Comment
<< Home