





Paroxysmal positional vertigo as a complication of osteotome sinus floor elevation
Eur Arch Otorhinolaryngol. 2005 Aug;262(8):631-3. Epub 2005 Feb 27.
Paroxysmal positional vertigo as a complication of osteotome sinus floor elevation.
Di Girolamo M, Napolitano B, Arullani CA, Bruno E, Di Girolamo S.
School of Dentistry, University of Rome Tor Vergata, Rome, Italy.
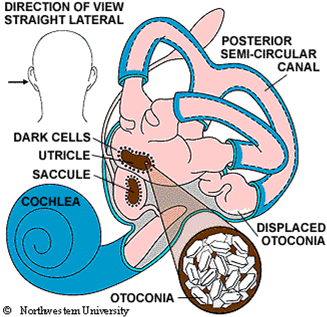
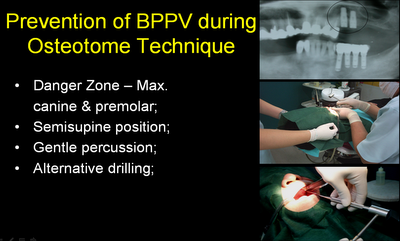
Paroxysmal positional vertigo (PPV) is a high prevalence, vestibular end organ disorder due to the detachment of the utricular otoconia floating in the posterior or lateral semicircular canal. Even though in the majority of cases the etiology of PPV is unknown, it may follow viral infection, vascular disorders and head trauma after different surgical procedures. The aim of this study was to investigate the correlation between PPV and the surgical trauma induced by the vibratory and percussive forces on the upper maxilla during the osteotome sinus floor elevation procedure. We performed a complete otoneurological examination on 146 patients affected by atrophic ridges before and after upper maxilla surgery. Four patients showed a PPV of the posterior semicircular canal controlateral to the implanted side 1 or 2 days after the surgical procedure, which promptly was solved with the Epley re-positioning maneuver. We hypothesize that the surgical trauma, and specifically the pressure exerted by the osteotomes, determines the detachment of the otoliths from the utricular macula while the patient head position, hyper-extended and tilted opposite to the side where the surgeon is working, favors the entry of these free-floating particles in the posterior semicircular canal of the implanted side. Although this disease is rather frequent in the normal population and it is a benign, self-limiting peripheral disorder, it should be considered by the oral surgeon as a possible complication of pre-prosthetic upper maxilla surgery, and the patient should be informed before undergoing surgery.
@ Clinical suggestions for preventing BPPV: (Dr. Perio had the BPPV after ridge expansion with Osteotome technique twice!)
 @ Dignosis and Therapy for BPPV: Epley maneuver
@ Dignosis and Therapy for BPPV: Epley maneuver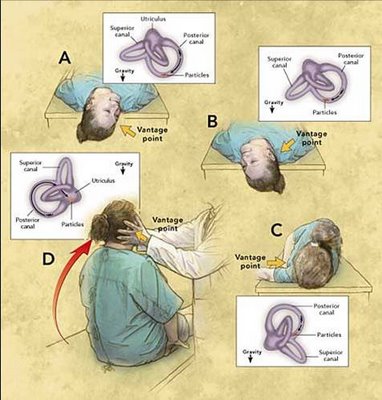
***Supplemental material on the site CD: Animation of Epley Maneuver.
Note that this maneuver is done faster in the animation than in the clinic. Usually one allows 30 seconds between positions
posted by Ajou Huang @ 11:35 am
0 comments
![]()
![]()
0 Comments:
Post a Comment
<< Home