





Bio-Col Socket Preservation Technique
 SOCKET GRAFT is indicated when the clinician wants to preserve the maximum amount of bone after tooth extraction. SOCKET GRAFT is designed to retain the alveolar ridge and speed bone fill into the socket. However,
SOCKET GRAFT is indicated when the clinician wants to preserve the maximum amount of bone after tooth extraction. SOCKET GRAFT is designed to retain the alveolar ridge and speed bone fill into the socket. However, 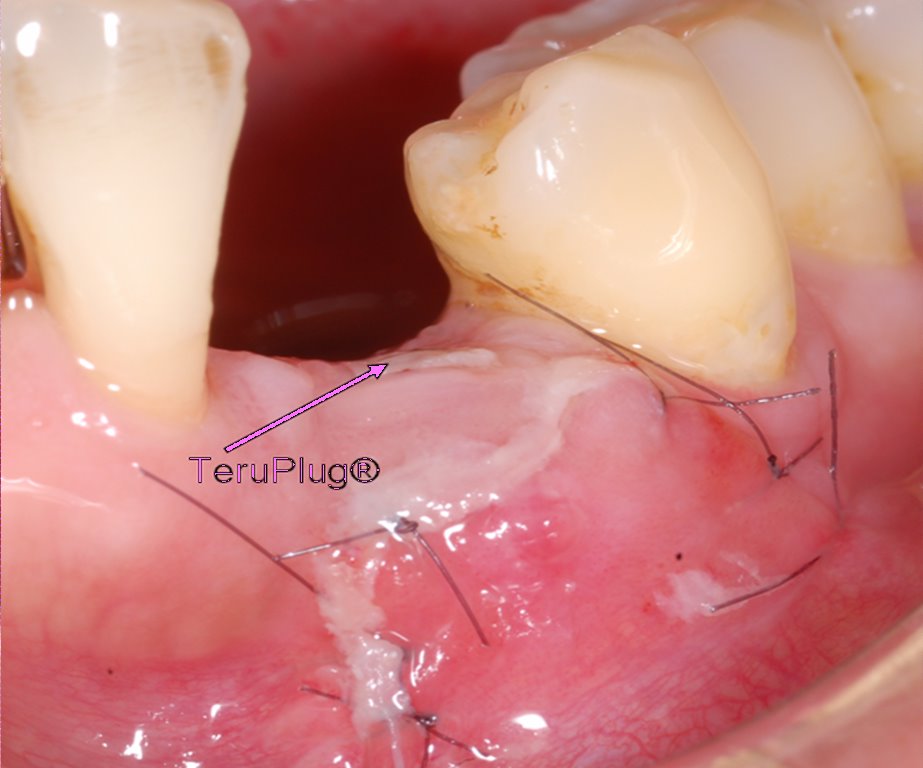 SOCKET GRAFT will not rebuild any part of the ridge lost prior to placement of SOCKET GRAFT. If the clinician knows prior to extraction that a significant amount of alveolar ridge is missing and more ridge is needed for implant placement or for esthetics then a ridge augmentation procedure is indicated with the use of hard bone graft material and the placement of a barrier to retain the graft.
SOCKET GRAFT will not rebuild any part of the ridge lost prior to placement of SOCKET GRAFT. If the clinician knows prior to extraction that a significant amount of alveolar ridge is missing and more ridge is needed for implant placement or for esthetics then a ridge augmentation procedure is indicated with the use of hard bone graft material and the placement of a barrier to retain the graft.Ridge Preservation for Optimum Aesthetics and Function. The primary goal of any ridge preservation technique should be to preserve both the hard and soft tissues, especially the interdental papillae, in such a way as to optimize aesthetics and function. The Bio-Col Socket Preservation Technique with an understanding of these goals and biological considerations, the "Bio-Col" socket preservation technique was developed. The surgical protocol ensures the preservation of both hard and soft tissues at the time of tooth extraction, and it virtually eliminates the bone resorption that would normally follow tooth removal.


1. Top View: Bleeding Extraction Socket with No Defect. Tooth is extracted atraumatically without flap reflection. Note intact bony walls of extraction socket and preservation of surrounding gingival anatomy.
2. Top View: Grafted Extraction Socket in Preparation for Conventional Prosthesis. Socket with intact bony walls is grafted up to alveolar crest with Bio-Oss® natural bone mineral. CollaPlug®* absorbable dressing is placed over the Bio-Oss® graft and sutured in place with a horizontal matress suture.
3. Buccal View in Transparency: Bio-Col Technique for Conventional Prosthesis. Socket with intact bony walls is grafted up to alveolar crest with Bio-Oss® graft material. CollaPlug® absorbable dressing is placed over the  Bio-Oss® graft and maintained with suture. A removable or fixed provisional restoration with an ovate pontic extending 3 mm to 4 mm subgingivally is placed, compressing the CollaPlug® and supporting the surrounding soft tissue.
Bio-Oss® graft and maintained with suture. A removable or fixed provisional restoration with an ovate pontic extending 3 mm to 4 mm subgingivally is placed, compressing the CollaPlug® and supporting the surrounding soft tissue. 
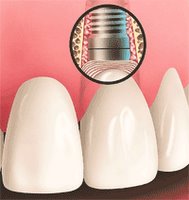
4. Top View: Bio-Col Technique With Immediate Implant Placement. Immediate implant placed into intact bony socket. Bio-Oss® bone mineral grafted between implant and bony socket walls. Implant fixture and Bio-Oss® graft covered with CollaPlug® absorbable collagen dressing. Horizontal mattress suture placed to maintain position of collagen wound dressing.
5. Buccal view in Transparency: Bio-Col Technique With Immediate Implant Placement. Procedure same as step 4 with the following addition: Tooth borne provisional restoration with a modified ovate pontic to avoid pressure over cover screw. Ovate pontic extends subgingivally to support surrounding soft tissues.
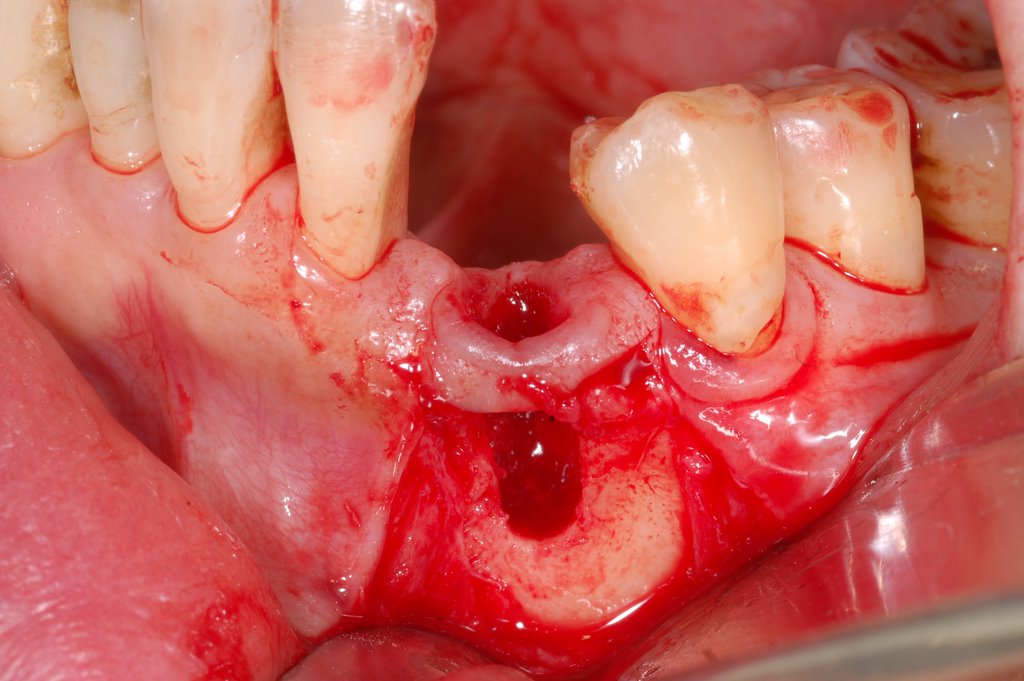
6. Top View: Compromised Extraction Socket With Buccal Wall Defect. After extraction, socket presents with a large buccal wall bone defect. Note the partial soft-tissue collapse into the defect area.

7. Top View: Grafted Compromised Extraction Socket in Preparation for Delayed Implant Placement or Conventional Prosthesis. After tooth removal, Bio-Gide® resorbable collagen membrane placed in prepared subperiosteal pocket, covering bony socket wall defect. Bio-Oss® bone mineral placed into the socket and defect area. Note that Bio-Oss® slightly expands the adjacent Bio-Gide® membrane and overlying soft tissues. CollaPlug® absorbable dressing is placed over the Bio-Oss® graft and maintained with suture.
8. Buccal View in Transparency: Grafted Compromised Socket in Preparation for Delayed Implant Placement or Conventional Prosthesis. Note Bio-Gide® membrane covering buccal wall socket defect. Procedure same as step 7 with the following addition: Provisional restoration with ovate pontic extending 3 mm to 4 mm subgingivally against CollaPlug® dressing, supporting surrounding soft tissues.
Clinical Case Report by Perio(Nov.05'):





.2.jpg)
 Apical /clinical checkup 3 months later<<
Apical /clinical checkup 3 months later<<
@Flapless approach for dental implantation after Bio-col ridge augmentation: (Surgery by Dr. Perio )



.4.jpg)
#Apicl check-up after dental inplantation (Mar06')

>>> 3 months later !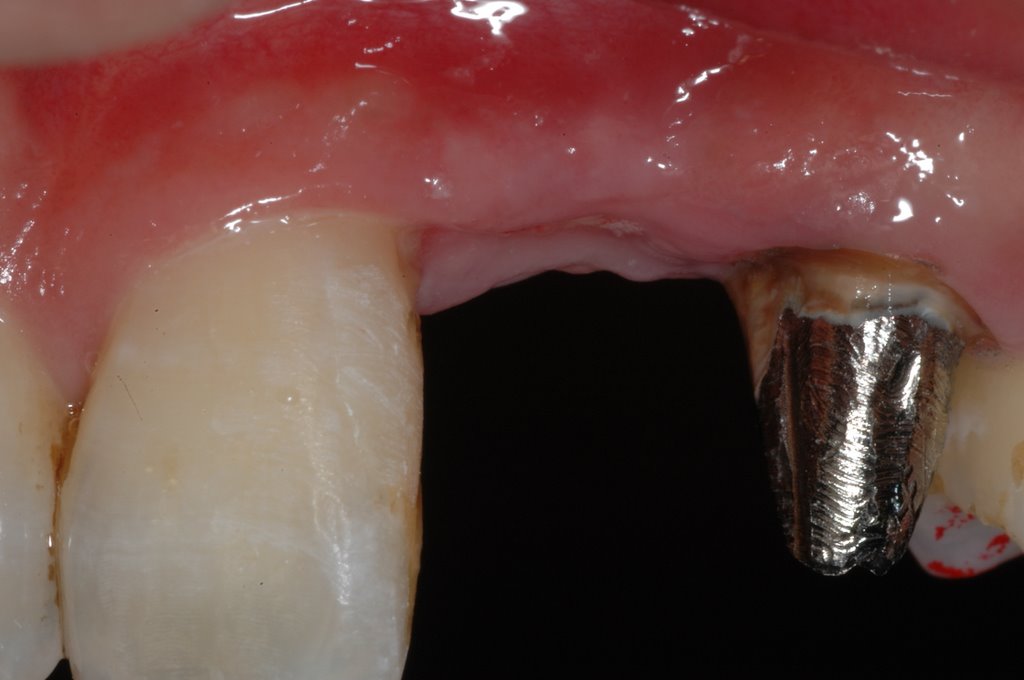

.3.jpg)
 @ Socket Augmentation: Rationale and Technique by Dr. Wang
@ Socket Augmentation: Rationale and Technique by Dr. Wang
@Free Article of Bio-Col ridge preservation technique
posted by Ajou Huang @ 6:53 pm
3 comments
![]()
![]()
3 Comments:
Hi sir:
Good question!
Bio-col technique for ridge augemntation + immediate implantation is suitable for buccal plate intact certainly.
But, the implant insertion with good primary stability without implant extrusion to alveolar house + easy buccal GBR with bone graft/membrane may indicate for this condition.
In my opinion the best technique when having to deal with a compromised extraction socket with buccal wall defect is the use of Bio-Oss Collagen + rhPDGFBB without any membrane. Study by Nevins (2009) showed excellent results using this technique and all 8 sockets with buccal wall defects showed bone formation and were able to support an implant after 4 and 6 months. The author suggests not to use a membrane in order to don't block periostal-based progenitor cells.
Article: "human histologic evaluation of mineralized collagen bone substitute and recombinant platelet-derived growth factor-bb to create bone for implant placement in extraction socket defects at 4 and 6 months: A Case Series" Int J Periodontics Restorative Dent 2009;29:129-139
Gianluca
Thank you Gianluca.
I will do that with membrane technique + bone grafting for ridge preservation after extraction.
Post a Comment
<< Home